
Case 25 - TB or not TB...
Author: Dr Salman Naeem Reviewer: Dr Nish Cherian
A 44 year old male presents with fever, night sweats, weight loss and a swelling over the left upper chest. This is his second presentation in 2 months, having previously presented with chest pain which was treated as musculoskeletal pain. He is originally from Pakistan, has no relevant PMH and denies any known TB contacts.
The swelling is tense, non-fluctuant, tender, cold and with no signs of erythema. He denies any cough.
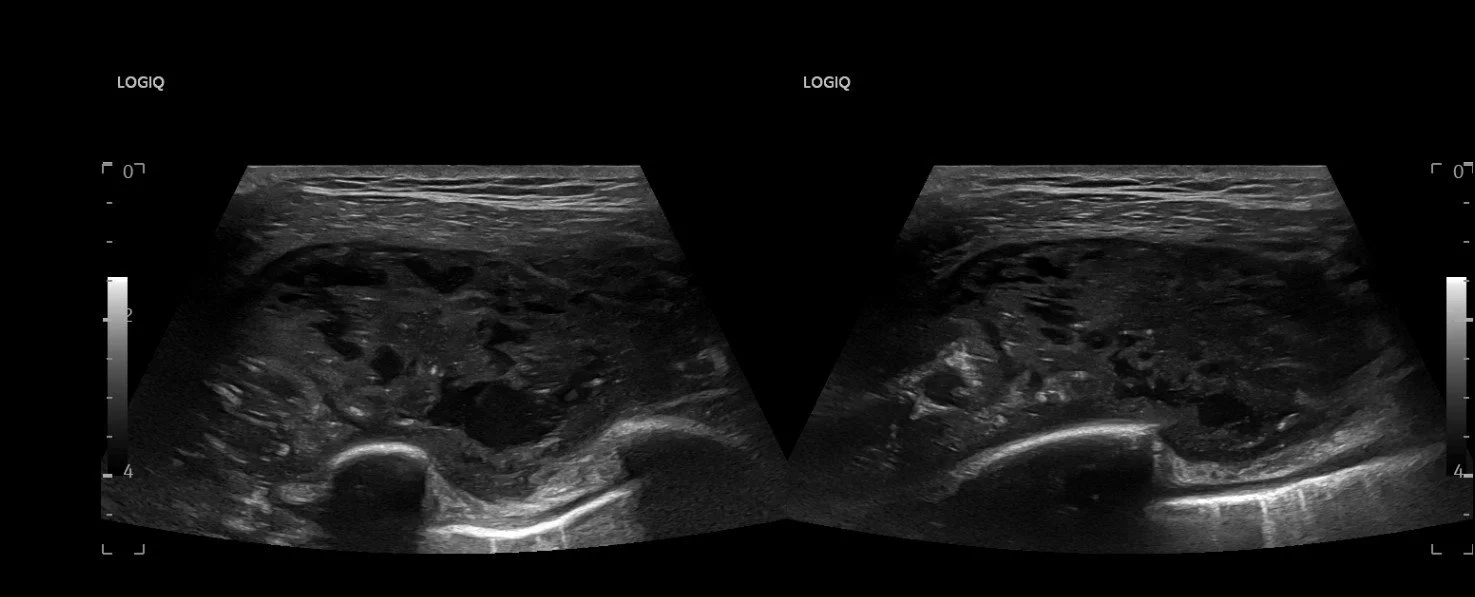
You decide to investigate it with an ultrasound scan showing the following:


Clip Collection (Press right/Left to change the clips)
-
US of the swelling demonstrates heteroechoic shadows in the pectoralis major muscle above the rib and pleura which can be seen deep to this, with pockets of hypoechoic fluid and a hyperechoic shadow. This is consistent with an abscess.
The ultrasound also shows oedema of the periosteum of the 1st rib, seen as the irregularity of the cortex. This is a periosteal reaction, a nonspecific radiological finding indicating periosteal irritation[1] that can be seen in osteal malignancy, infection or trauma, amongst other things.
-
Given the history and background, this is most likely a ‘cold abscess’ in the context of Mycobacterium tuberculosis infection.
CASE RESOLUTION
The departmental ultrasound report noted: “The left pectoralis major intramuscular collection demonstrated heterogeneous echotexture with mostly solid looking components and scattered anechoic cystic regions.”
Given the history, ultrasound and examination findings, the patient was diagnosed with TB osteomyelitis and a cold abscess which was later confirmed on CT. He was started on anti-tuberculous medications within 24 hours due to his expedited diagnosis.
POCUS Assessment of Skin/Soft Tissue Infections in the ED
Ultrasound is an excellent imaging modality for superficial skin and soft tissue infections, with a sensitivity of 97%, specificity of 83% and positive LR of 5.5[2]. This surpasses clinical examination alone in the diagnosis of abscesses in the Emergency Department and there are studies suggesting that abscess measurements on ultrasound may have a role in directing conservative vs surgical management and predicting success or failure of such approaches[3].
When assessing soft tissue with ultrasound, it is useful to visualise local or contralateral side normal tissue in order to compare appearances.
Normal soft tissue appearances on ultrasound are as follows:
Fat appears hypoechoic with interspersed hyperechoic linear echoes running mostly parallel to the skin, representing connective tissue septae.
Fascia appears as a linear hyperechoic layer.
Muscle fascicles can be visualized as hypoechoic cylindrical structures, with hyperechoic connective tissue surrounding them

CELLULITIS
Early appearances of cellulitis may be generalized swelling with increased echogenicity of the skin and subcutaneous tissues. As cellulitis progresses and the amount of subcutaneous fluid increases, hyperechoic fat lobules become separated by hypoechoic/anechoic fluid-filled areas. This later stage of cellulitis is most typical and has been described as having a “cobblestone appearance”.
Early cellulitis (left) with normal tissue (right):

Later cellulitis with “cobblestone appearance”:

Abscesses/cysts appear as well demarcated hypoechoic/anechoic fluid-filled areas (depending on the content). An assessment of the fluctuance of an abscess and hence suitability for drainage can also be performed to guide management.
A good review on soft tissue and abscess evaluation from the American College of Emergency Physicians (ACEP) can be found here.
REFERENCES