
Case 18 - No Time For Hips to Lie
Author: Nick Mani Reviewer(s): Nish Cherian
A 90-year old male presents with a fall and sustains a right neck of femur fracture. She has been given IV paracetamol and morphine but continues to be in pain and discomfort. The relatives and nurses are requesting more analgesia. The Trauma & Orthopaedic specialist is asking for better pain management before transfer to the ward.
You elect to perform an ultrasound-guided compartment block as part of a multi-modal pain management strategy as shown below: -
Clip 1- Right Inguinal Region (Left- Lateral, Right- Medial)

Image 1- Sono-Anatomy of the Performed Block
-
Infra-Inguinal Fascia Iliaca (IIFI) compartment block
Compared to the newer approach of taught Supra-Inguinal Fascia Iliaca (SIFI), it is a distal approach to blocking the nerves in the compartment (femoral, lateral cutaneous, and obturator). The needle tip is going towards the femoral vessels and much deeper, making it an overall less effective and safer approach as shown in the literature.
-
Performed within 6hrs of the same/similar block
Infection over/around the injection site
Open wound at the site of injection/Intravenous drug user with acive injection site
Vascular surgery such as a bypass
NB anticoagulation/potent antiplatellets are ONLY a relative contraindications, much more so for supra- compared to infra-inguinal FICB. It is an absolute contraindication when the procedure is performed anatomically/blind (https://www.ra-uk.org/images/Documents/RAPAC_for_consultation.pdf)
-
A - Fascia Lata
B - Sartorius Muscle
C - Fascia Iliaca
D - Hydro-dissection/Local Anaesthetic
E- Femoral Nerve
F- Iliopsoas muscle
G- Femoral Artery
-
Recording of vital signs every 5 minutes for a total of 30 minutes.
Due to possibility of opioid toxicity from removal of the pain stimulus post-block.
-
Perineural (preservative free) or IV dexamethasone (max dose 8mg) could be considered and has shown to significantly increase the duration of various nerve blocks in the Anaesthesia literature (https://doi.org/10.1097/ALN.0000000000004557)
A 2017 systematic review would suggest perineural dexamethasone combined with bupivacaine to be more effective than systemic (https://doi.org/10.1093/bja/aex191)
-
Needle visualisation setting to steer the beam
SONO-ANATOMY & TECHNIQUE
Infrainguinal fascia iliaca compartment - scanning approach
Place the probe over just under and parallel to the inguinal ligament in the lateral half. Slide the probe medially along the same plane along to identify the neurovascular bundle.
The femoral artery will be obvious as the most round and pulsating vessel and medial to this lies the femoral vein (remember NAVY). However, the femoral nerve is not often easily visualised yet until it has local anaesthetic around it and separated from the fascia and fat. Slide the probe slowly laterally and adjust by rocking until there is a clear demarcation of the sartorius muscle with fascia lata and iliaca on either side, with the iliopsoas muscle in the far field.
Insert the needle in-plane with the transducer. Inject the local anaesthetic just under the fascia Iliaca and observe the hydro-disection as shown. Note that this is NOT a femoral nerve block, but a compartment block- therefore the aim is to stay away from the nerve and administer the anaesthetic under the fascia iliaca which spreads along the compartment to block the main nerves innervating the hip (femoral, obturator and lat. cutaneous nerve of thigh). This requires adequate VOLUME for good coverage- hence using around 30-40ml total volume in most patients (you can dilute further with saline if more volume required).

Image 2 - Surface Anatomy of Different Hip/Pelvis Blocks
FICB (II)- Fascia Iliaca Compartent Blcok Infra-Inguinal, FICB (SI)- Fascia iliaca Compartment Block Supra-Inguinal, FN- Femoral Nerve Block, PENG- Peri-Capsular Nerve Group Block

Image 3 - Infar-inguinal (II) Fascia Iliaca Compartment Block (FICB) (Anterior Pelvic Skeletal View)
ASIS- Anterior Superior Iliac Spine, LFCN- Lateral Femoral Cutaneous Nerve, FN- Femoral Nerve, ON- Obturator Nerve

Image 4- Ergonomicology/Safety
Patient, Performer, Assistant, Equipment, Monitoring, Check-list/Stop Before You Block
Note- the ultrasound machine is at the opposite side of the bed for this block
Clip 2 - Sono-Anatomy of the Performed Block with Annotations
FL- Fascia Lata, FI- Fascia Iliaca, LA- Local Anaesthetic, SM- Sartorius Muscle, IP- Iliopsoas Muscle, FN- Femoral Nerve, FA- Femoral Artery
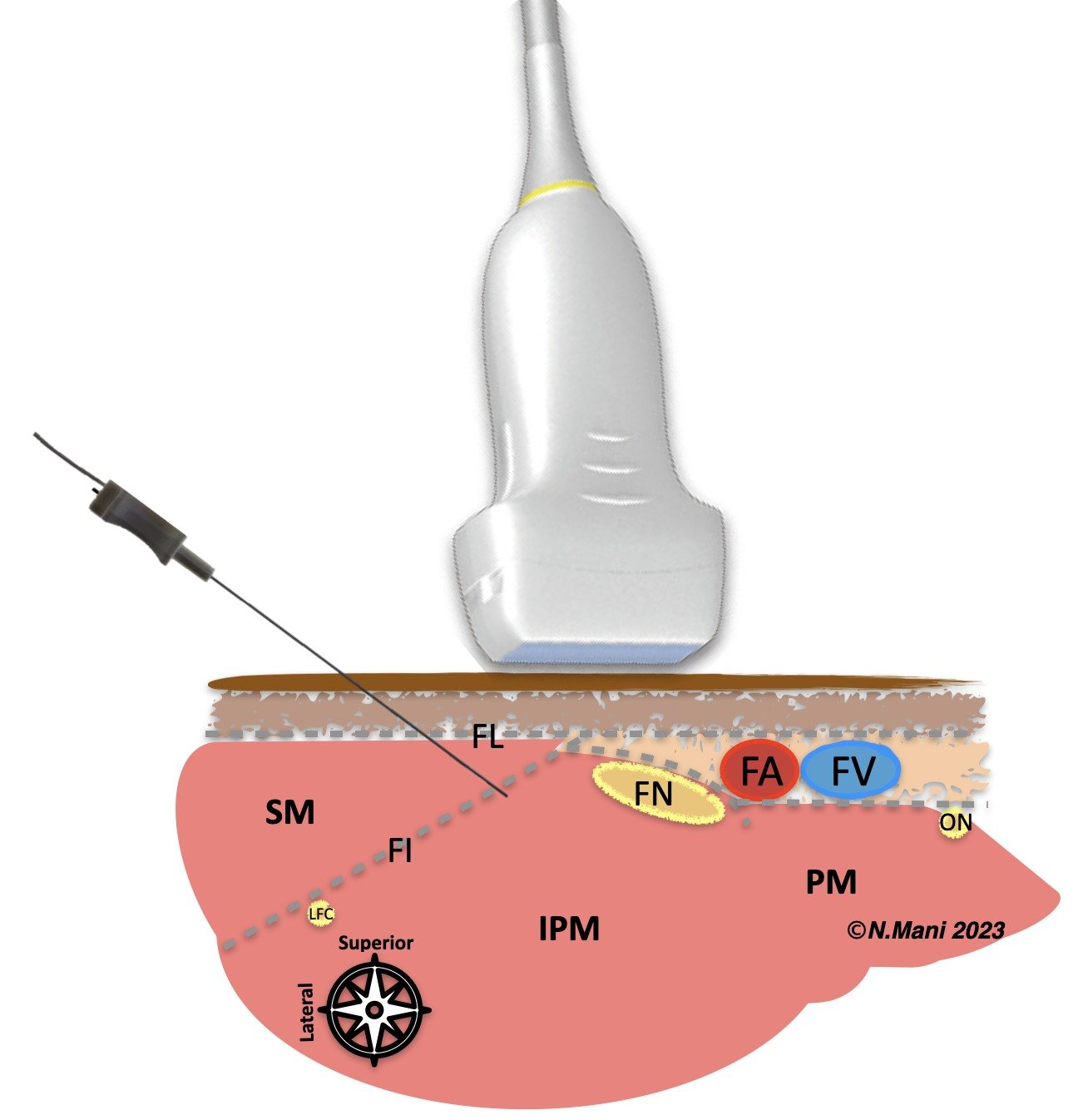
Image 5- Cartoon demonstration of Fascia Iliaca Compartment Block (FICB) Infra-inguinal (II) In-Plane
SM- Sartorius Muscle, IPM- Iliopsoas Muscle, PM- Pectinous Muscle, FL- Fascia Lata, FI- Fascia Iliaca
FN- Femoral Nerve, FA- Femoral Artery, FV- Femoral Vein, ON- Obturator Nerve, LFC- Lateral Femoral Cutaneous Nerve
Case resolution
The patient had effective analgesia with the US-guided infra-inguinal fascia iliaca block and did not require any further analgesics. The patient was admitted to the orthopaedic ward overnight and operated on the following day.
Take home message
Ultrasound guided FICB is easy to learn and perform. Suprainguinal approach is now the preferred approach (see pocusuk.org/cases/hips-don’t-lie), however infrainguinal approach is still widely acceptable and practiced.