
Case 17 - I've Got Your Back!
Author: Gokul Sagar Bailur Reviewer(s): Nick Mani/Nish Cherian
An 80-year old male presents to ED after a fall down the stairs, sustaining multiple posterior and lateral rib fractures with haemothorax on CT. He has been given IV paracetamol and morphine but continues to be in significant pain, unable to deep breathe, cough or mobilise.
You elect to perform an ultrasound-guided regional anaesthetic as part of a multi-modal pain management strategy.


-
Erector Spinae Plane block (ESPB)
-
Mainly posterior lateral rib fracture, however it is thought to also cover the anterior rib fracture as what it thought as the ultimate Plan A block.
-
Performed within 6hrs of the same/similar block
Infection over/around the injection site
Open wound at the site of injection
NB anticoagulation/potent antiplatellets are ONLY a relative contraindications (https://www.ra-uk.org/images/Documents/RAPAC_for_consultation.pdf)cription
-
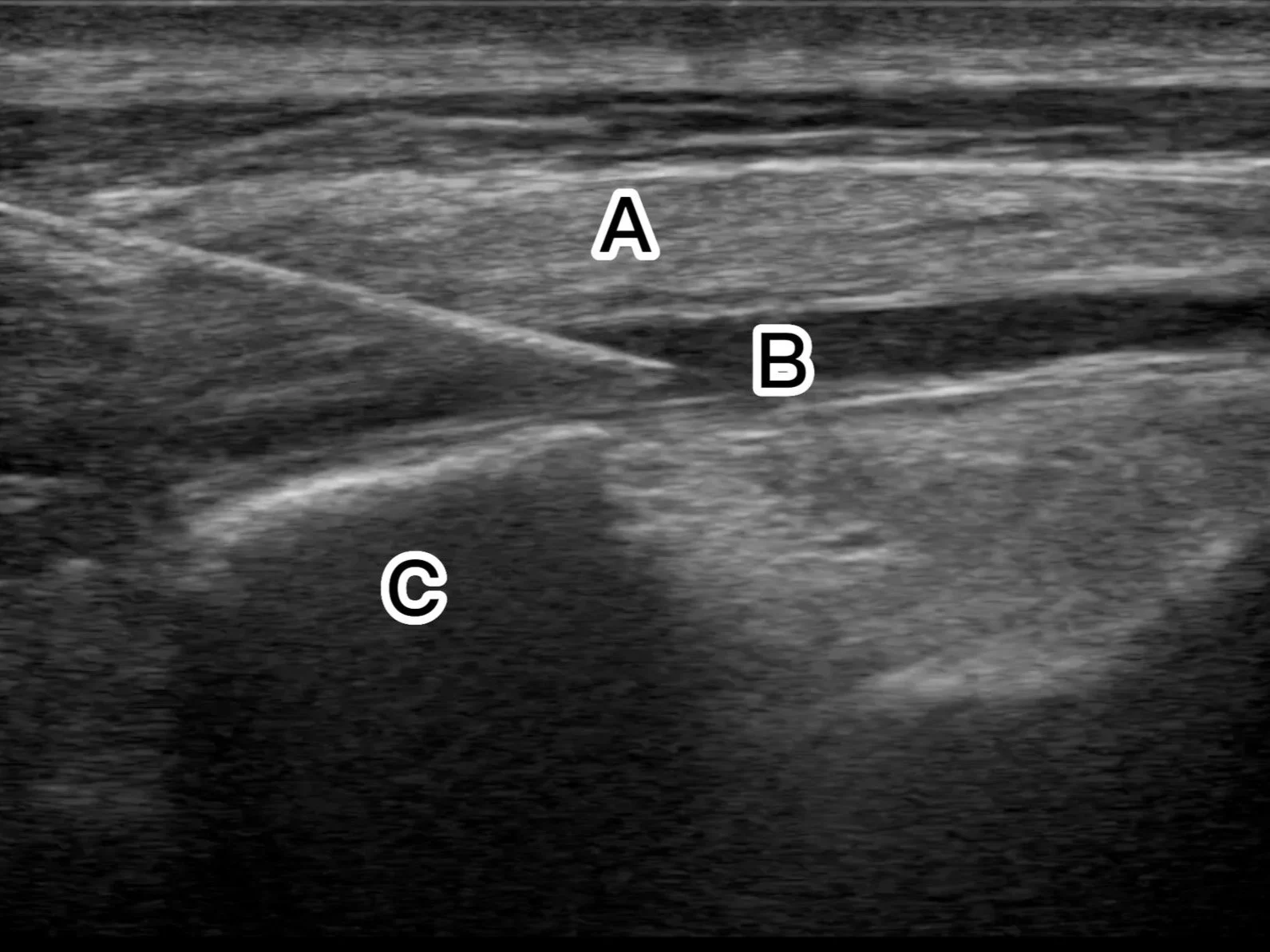
A - Ribs
B - Hemothorax
C - Pleura
-
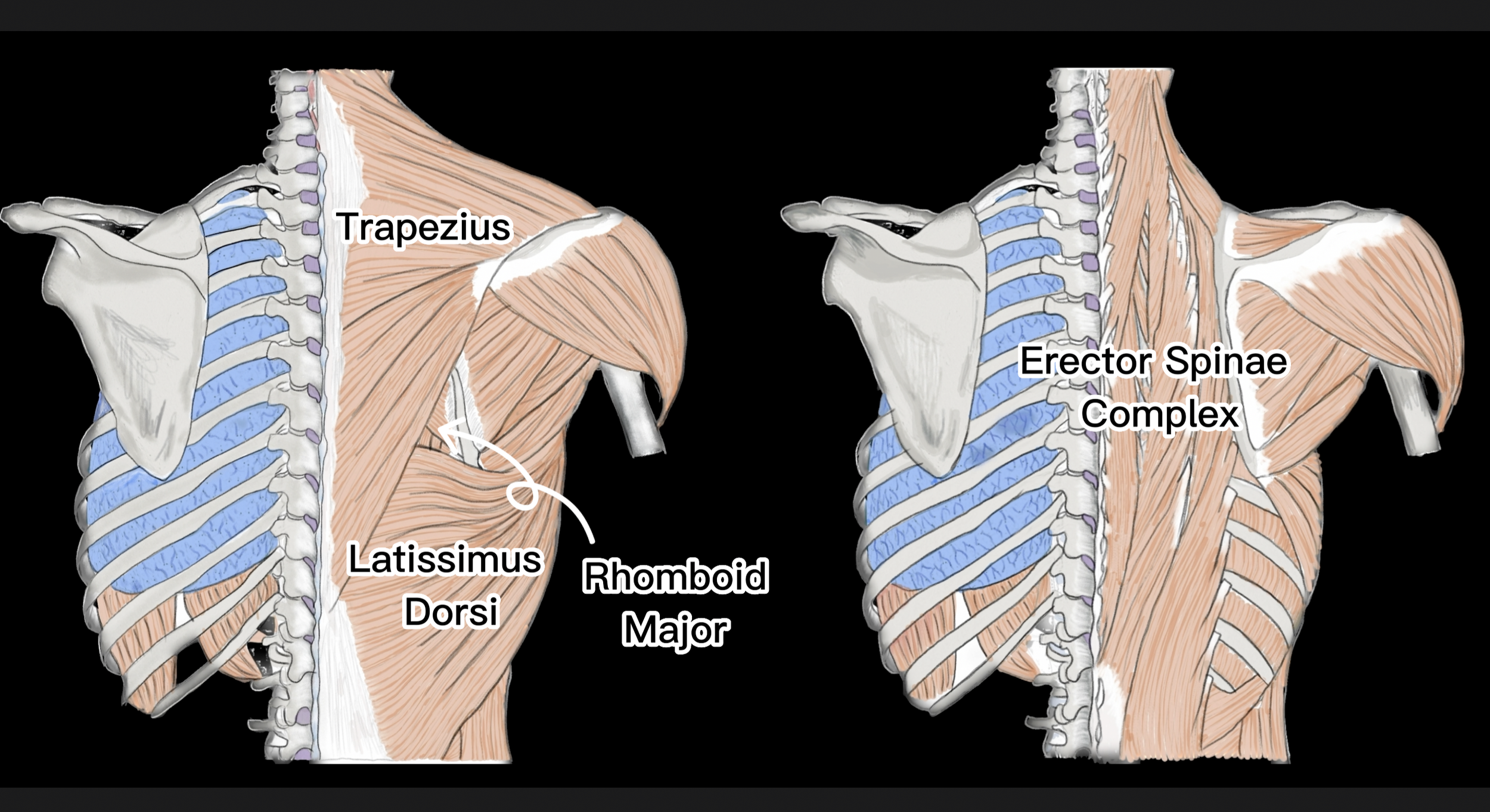
A - Erector Spinae muscle
(Trapezius & rhomboid major muscles might be visualised too, visualised as a three layer muscle complex)
B - Local anaesthetic
C - Transverse Process
-
3.3mg peri-neural dexamethasone mixed with the local aneasthetic (ideally preservative free), or 6.6mg IV dexamethasone
-
BATTLE Score
This patients BATTLE Score was 32. This indicated that there is about 88% chance of developing complications such pneumonia, atelectasis, respiratory failure and/or requiring critical care admission.
-
Serratus Anterior Plane Block (SAPB) Case 7
(ESPB could still be used for anterolateral rib fractures as well)
-
After 6hrs, and as long as within the safe total local anaesthetic dose calculate with patient weight.
Sometimes a catheter could be inserted into the space for continuous infusion, however in setting such as emergency department there is a high chance of this becoming infected and is not recommended.
SONO-ANATOMY & TECHNIQUE
General Approach to Scanning for ESP Block
The patient can be positioned either sitting up or lateral decubitus position.
The linear (or curvilinear depending on the body habitus) probe is placed in a cranio-caudal orientation just medial to the scapula. It is usually at the level of the 5th rib or lower depending on the level of the rib fractures (as a plane block usually covers 3 rib levels cranial and caudal from the injection site level). This level could be located by counting down the ribs either manually, or with ultrasound visualisation.
Visualise the ribs which have a rounded contour and underlying pleura. Slide the probe medially towards parasagittal plane, and carefully look for transition of the rounded ribs to a tombstone/square-shaped transverse process (TP) of the spine.
Insert the needle either cranially or caudally aiming for the TP either corner/tip with the aim of injecting local anaesthetic +/-dexamethasone just below the Erector Spinae muscle, lifting the muscle off the TP. 5-10ml of saline could be first injected to open up the plane.


Case Resolution
The patient’s pain dramatically improved following the block and he was able to deep breathe, cough and mobilise. The patient was admitted under the Thoracic surgery team for further assessment and management.
Take Home message
Single shot ultrasound guided ESPB is effective and safe in patients with posterolateral (and anterolateral) multiple rib fractures.
Appendix